content warning: Discussion of anatomy of body parts related to sexual function, including the oh-so-naughty words “urine,” “penis,” and “semen” and even a drawing showing body parts. You’ve been warned
My medical school class was 50%+1 women. Many of them, when we were studying the urogenital system, made a complaint along the lines of “god made the female urethra too short.” Women, you see, are much more prone to urinary tract infections (UTI, often referred to as a “bladder infection”) than men. Men don’t get them nearly as often. The short urethra is more prone to allowing bacteria to enter the urinary tract and get established and cause an infection before urine flow washes it out. UTIs can be spontaneous, but are more likely following sexual activity.
Why is there bacteria around? Because “Love has pitched his mansion in/The place of excrement.”
The male urethra, on the other hand, is longer and more tortuous, having to traverse the length of the penis, then go through a gland called the prostate (which functions to produce semen), and only then into the bladder. That means there’s much more opportunity for pathogenic bacteria to get washed out by urine flow before it can latch on and infect the tissues higher in the urinary tract.
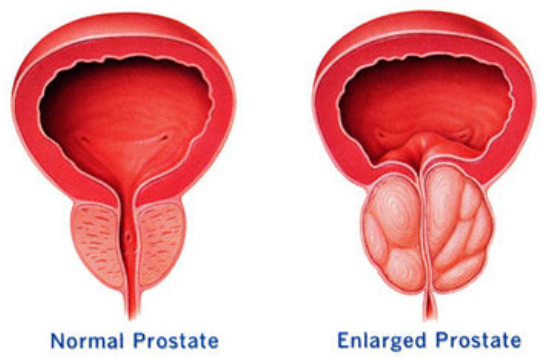
The twentysomething young proto-doctors in my class, while wishing for longer urethras, weren’t thinking about the other end of the bargain. The longer male urethra is subject to restriction (yes, just like the evil flow restrictor on my new kitchen faucet). This usually happens because the prostate grows over time, so many Men of a Certain Age start experiencing a host of inconvenient, sometimes painful, and usually “not discussed in polite company” symptoms like sudden, extreme urges to urinate; difficulty urinating; needing to urinate frequently; difficulty initiating urination; and incontinence. Ewwww.
I have had relatively mild symptoms of an enlarged prostate (“benign prostatic hypertrophy” or BPH) since my teens, but they have worsened and become problematic with the passage of time. Treating this condition is largely the purview of urologists, a specialty with which I have a complicated history. So I put off definitive treatment as long as I could. I have been taking medications that can mitigate the symptoms, but not indefinitely and the symptoms are now impacting my quality of my life. (Hey, I made it half a century so I think I did pretty well.)
When I was in medical school, the treatment of choice for BPH was a procedure known as a “transurethral resection of the prostate” or TURP, often colloquially referred to as a “Roto-Rooter” procedure. It involves inserting surgical instruments into the urethra up to where it passes through the prostate, and scraping away the tissue of the prostate from the inside. This is done under anesthesia but still seems unpleasant. There are newer procedures that, like the TURP, are performed by urologists, usually in their offices or a same-day surgery center. All have various degrees of risk for incontinence, impotence, or treatment failure. They all have the side effect of reducing ejaculatory volume which — in spite of some medical professionals’ assertions to the contrary — can be important even to ancient men in their sixties.
There is another treatment that is generally not performed by urologists (urology is a surgical speciality), but by interventional radiologists. That’s the prostatic artery embolization (PAE) that I’m scheduled for tomorrow. It involves inserting a catheter (a long flexible tube) into the big artery in the groin. The radiologist then watches on a fluoroscope (yes, just like the ancient days, but using modern technology to make images using far less radiation) while they advance the catheter to the artery that supplies blood to the prostate. They then inject a device or material that causes the blood to clot. That reduces blood flow to the prostate which, if all goes according to plan, causes the gland to stop growing and instead to shrink a bit over time. There are still risks, but the risk of incontinence and impotence seem to be much smaller. The risk for treatment failure (symptoms fail to improve) is higher than with surgical procedures. I believe (but haven’t seen documented) that the risk for reduction in ejaculatory volume is smaller than for the other procedures.
You may not have heard of PAE. It occupies kind of a strange niche, as urologists are accustomed to performing their own procedures. Referring out to radiologists means they lose the confidence that comes with familiarity, they lose control, and of course they also lose revenue. So, for understandable reasons, urologists tend to be dismissive of PAE. In my limited experience, though, interventional radiologists take a patient-centric approach to their practices that I find reassuring, so I went out of my way to find an IR who specialized in PAE.
If all goes to plan, I’ll have the procedure tomorrow but it will be some weeks before we’ll know if it’s successful.
—2p
addendum 2026-06-11T19:55-07:00
The procedure went long, but I’m back “home” and recovering. The clinical experience was about as pleasant as could be imagined. I’m in a bit of pain and woozy from anesthesia, so I’ll write no more until I’m more fully recovered. It will be a couple of months before we know if the procedure was successful.
addendum 2026-06-13T16:16-07:00
So far, the recovery isn’t going so well.